Tattoo Ink - Where Does It All Go?
|
At A Glance
|
|
|
Author
|
Geranyl
|
|
Contact
|
|
|
IAM
|
|
|
When
|
N/A
|
Disclaimer:All
images here are rough representations. Please read the text, not just the
caption, for a full explanation. Also, the information presented here is
in no way guaranteed to be complete, however I have tried to piece together
as much of the puzzle as possible. Feel free to contact me if errors or
omissions are found.
Contents:
Introduction
Jargon - feel free to skip this section, but it may be useful
to refer to while reading the text
The Skin
- Epidermis
- Dermis
Tattoo Ink Placement
Stages of Ink Dispersal
- Then why does the tattoo fade over time?
- What about the sun?
Tattoo
ink dispersal in the skin has not been thoroughly studied despite the long
history of tattooing. The following is whatever I have managed to piece
together from journal articles and textbooks. For those of you who would
like to read the original science jargon, or to read about different ink
particle sizes (depends on the colour) check out these links:
Tattoo
Ink Removal - Covers the Location of Tattoo Ink and Ink Particle Sizes
A
Lecture About Skin - Covers Cellular Detail
These
are some definitions that may be useful.
Extracellular
- outside of the cell
Intracellular - inside the cell
Phagocytosis - think of it as the cell swallowing an
item e.g. a particle of tattoo ink
Phagocytic - cells that are capable of phagocytosis;
some cells can become phagocytic during an inflammatory response (e.g.
keratinocytes), whereas others are phagocytic all the time (e.g. many immune
cells).
Dendritic Cell - an immune cell type that continually
samples its environment for changes, and will migrate to lymph nodes to
trigger an immune response if necessary.
Mast Cell - an immune cell that plays a crucial role
in allergic reactions and is present in connective tissue.
Extracellular matrix - a generic name for the scaffold
of proteins (both structural and "glue" types) that cells attach to and
are supported by. Major components include basement membrane (one type
of collagen network), elastic fibers, structural glycoproteins (e.g. fibronectin),
proteoglycans("glue") and collagen.
Fibrocyte - a cell type that makes up most of the cells
in connective tissue. They secrete collagen as well as other proteins that
make up the extracellular matrix when activated. They are not normally
phagocytic, but become so when inflammation occurs.
Fibroblast - a fibrocyte that is actively secreting proteins
(an active fibrocyte).
Granulation tissue - tissue that fills in gaps formed
from debris or necrotic tissue removal. It consists of newly formed small
blood vessels embedded in a loose structure of fibroblasts and immune cells.
As the tissue matures, immune cells decrease in number, fibroblasts form
collagen networks and blood flow resumes to the area.
The Skin
The skin is made up an outermost layer named the epidermis, followed by the dermis and the hypodermis.
·Epidermis: composed mostly of keratinocytes, cells that contain keratin, the protein that gives skin its toughness (not to be confused with collagen which gives skin its resiliency).
·Dermis: a network of elastic dense connective tissue containing collagen as well as sweat glands, hair follicles, sebaceous ("oil") glands, nerve endings and blood vessels.
·Hypodermis: loose connective tissue containing mostly adipose (fat) tissue.
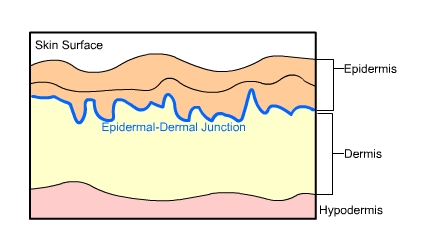
Fig.1 The Three Layers of the Skin
Epidermis
The
epidermis is separated from the dermis by a basement membrane (an extracellular
network of collagen fibers that serves as a support framework for cells)
that strengthens the interface between the epidermis and dermis to prevent
tearing from excessive stretching.
There are five layers of the epidermis, where the surface layers are regenerated from stem cells in the deepest layer that differentiate as they move outwards:
·Stratum basale (deepest)
·Stratum spinosum
·Stratum granulosum
·Stratum lucidum
·Stratum corneum (surface)
Briefly, the stratum basale contains keratinocyte stem cells ("basal cells") that are continually dividing to create new cells. These cells differentiate, or in other words change, as they migrate through the layers to the surface. The stratum granulosum is the "waterproofing" layer of cells, and cells no longer divide at this level. The outermost surface layer is composed of dead keratinocytes which are essentially cells filled with keratin.
Dermis
The
dermis, a connective tissue made up of collagen and networks of elastic
fibers which give skin its resiliency, is the layer in which tattoo ink
is deposited. The dermis (papillary layer) immediately below the epidermis
is made of loose connective tissue and contains small blood vessels and
nerve endings. The rest of the dermis (reticular layer) is made of dense
connective tissue and contains blood vessels, hair follicles, sweat glands,
lymphatics, nerves, and sebaceous glands.
The
majority cell type in the dermis is fibrocyte (or fibroblast). These cells
secrete the proteins that make up the connective tissue network. Other
cells that are important in relation to tattoo ink are resident immune
cells. These include dendritic cells, macrophages, and mast cells.
Tattoo
Ink Placement
The
tattooing process causes damage to the epidermis, epidermal-dermal junction,
and the papillary layer (topmost layer) of the dermis. These layers appear
homogenized (or in other words, like mush) right after the tattooing process.
The ink itself is initially dispersed as fine granules in the upper dermis,
but aggregate into more concentrated areas at 7-13 days.
Like
any injury, the initial response is to stop bleeding, followed by tissue
swelling, and the migration of non-resident immune cells into the area.
The "automatic response" immune cells are mostly neutrophils, and macrophages
later on. They are phagocytic cells that "swallow" debris to clean up the
area and then leave via the lymphatics. This is the extent of an immune
response unless an allergic reaction occurs or an infection sets in. The
tissue is then repaired and/or regenerated by fibroblasts. Initially the
tissue formed is known as granulation tissue (think fresh scar, pinkish
and soft), which later matures into fibrous tissue (think old scar).
Stages of Ink Dispersal
Initially ink is taken up by keratinocytes, and phagocytic cells (including fibroblasts, macrophages and mast cells).
At one month the basement membrane of the epidermis (epidermal-dermal junction) is reforming and the basal cells contain ink. In the dermis, ink containing phagocytic cells are concentrated along the epidermal-dermal junction below a layer of granulation tissue that is surrounded by collagen. Ink is still being eliminated through the epidermis with ink present in keratinocytes, macrophages and fibroblasts.
At two to three months the basement membrane of the epidermis is fully reformed, preventing any further loss of ink through the epidermis. Ink is now present in dermal fibroblasts. Most of these ink containing fibroblasts are located beneath a layer of fibrous tissue which has replaced the granulation tissue. A network of connective tissue surrounds and effectively traps these fibroblasts. It is assumed that these fibroblasts are the cells that give tattoos their lifespan.
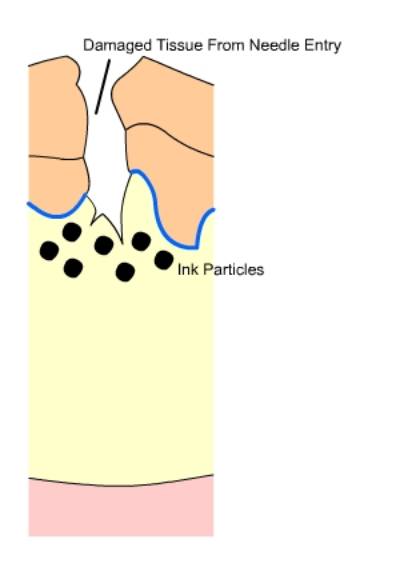
Fig.2 Injured Tissue: Ink is deposited into the upper surface of the
dermis upon needle entry.
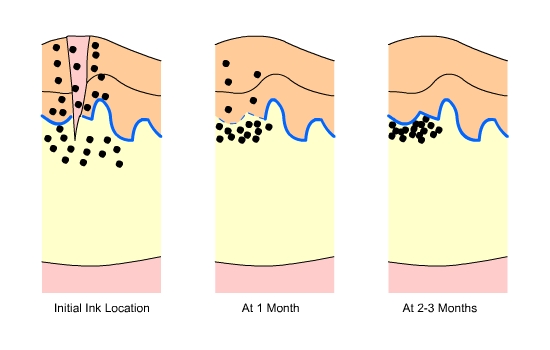
Fig.3 Ink Location: soon after the tattoo is received, one month after,
and two to three months after. Note the reformation of the epithelial-dermal
junction over time and the concentration of ink just underneath it.
Then why does the tattoo
fade over time?
What
about the sun?
Sun
exposure equals sun damage, whether you realize it or not. Langerhans cells,
a type of dendritic cell, are present throughout the epidermis, but mostly
located in the stratum spinosum. During sun exposure, many Langerhans cells
will undergo apoptosis (a type of cell death where the cell breaks apart
into many small fragments) while others migrate into the dermis and a minor
inflammatory reaction occurs. The inflammatory reaction is not restricted
to the epidermis, but also involves the dermis. Such a reaction causes
the recruitment of more phagocytic immune cells to the area.
With
the presence of larger than normal amounts of migrating phagocytic cells,
the chances of ink movement increases, thus accelerating the fading of
the tattoo.
Compiled:
January 13 2003
been edited. We can not guarantee that the experience is accurate, truthful,
or contains valid or even safe advice. We strongly urge you to use BME and
other resources to educate yourself so you can make safe informed decisions.